PIECEs Newsletter 3 – Dec 2021/Jan 2022
Our end of the year newsletter is out! Make sure you read it here




Community Engagement – Theory of Change workshops in Pakistan
*Text by Hufsa Sarwar, PIECEs Research Coordinator
When our team first started brainstorming ideas around engaging the wider community through the PIECEs project, we were very clear on one thing: it was imperative to put the voices and experiences of people with lived experience of psychosis front and center and make sure that our engagement strategies are relevant and representative to our stakeholders and target populations. This sentiment is echoed through the rest of activities taking place within the project; the Lived Experience Advisory Panel which overlooks and guides the research team, the Theatre of the Oppressed workshops involving people with psychosis and caregivers, and the adaptation of the DIALOG+ app based on feedback from both services users and healthcare providers. We therefore decided to hold a Theory of Change session with a group of people with psychosis, caregivers, and healthcare providers in Pakistan to identify key challenges to support contextual solutions, and to build capacity towards a user-led and participative approach to mental health research and advocacy.

Theory of Change (ToC) is essentially a method which aims to explain how different components of a programme can lead towards a specific impact or the required change. It works on mapping out the various outcomes, interventions, indicators, rationales and assumptions one needs to be aware of to properly design and implement an evidence based programme or strategy. Since our group consisted of people with differing academic and educational experiences and backgrounds, we tried to simplify the concepts and focus the discussion around the experiences and wishes of our stakeholders within the existing system and communities that they inhabit. Co-production is a novel concept in mental health programming for psychosis within Pakistan, and taking a lead in planning different aspects of a major programme even more so for our participants.

Initially, many seemed confused; however, when the research team started asking them about their daily experiences they bloomed and started expanding upon the challenges they faced, and to which they desperately wanted solutions. People with psychosis shared that they wanted to have better treatment outcomes, achieve independence and self-reliance in their overall lives, and be able to integrate within a society which was better educated on their condition. Healthcare workers discussed how they wanted to see a visible impact on healthcare systems, with more accountability and efficient methods in place. The caregiver group, which was extremely passionate and invested in the discussion, said that they wanted to see their family members with psychosis thrive and be able to contribute meaningfully to society, and lead happier and healthier lives. They also stated the importance of accessibility to mental health services for all – caregivers need extensive support as well, along with increased social engagement and reduced stigma for both people with psychosis and their families.
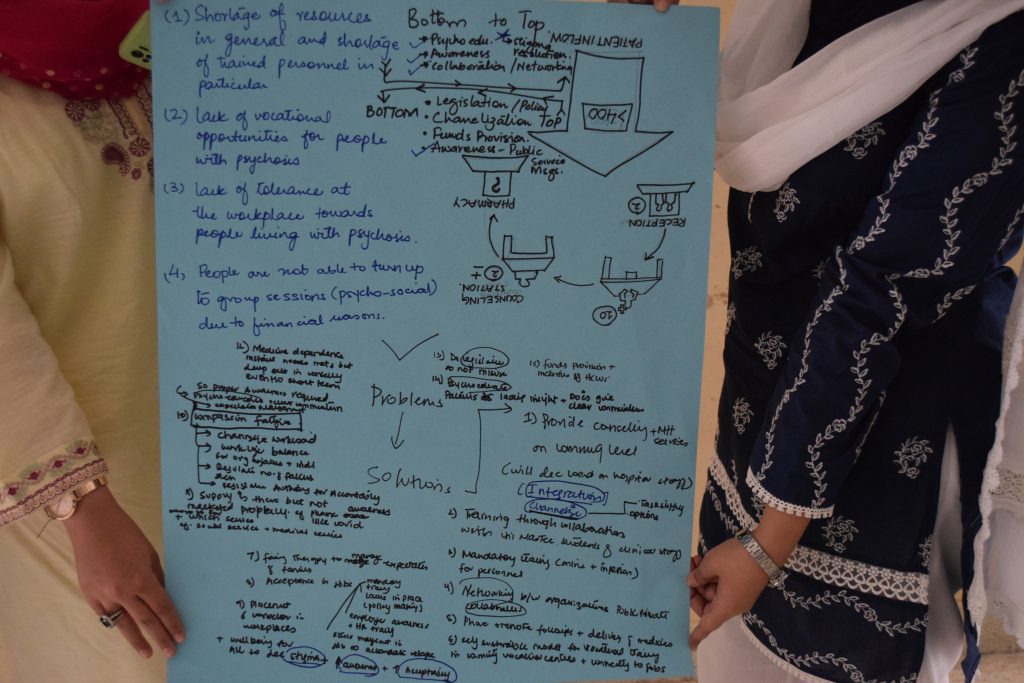
The two-day session opened our eyes to many of the hidden challenges that all three stakeholder groups face; it was also a space for them to share their own thoughts around potential solutions for these issues. This was an opportunity for both the research team and participants to start developing a co-produced model for community engagement with effective, equitable, and appropriate packages of care which can utilise and strengthen access to community resources and break through the existing power dynamics. We hope to continue engaging with the wider community and amplify their voices as we start implementing our interventions.
PIECEs: Arts workshops at the HINDU Times
Sanjoy Ganguly, pioneer of Theatre of the Oppressed in the country, was recently in Chennai for a workshop with SCARF India, as part of PIECEs research
You can read the article here


Interview with facilitators: Arts Workshops as part of PIECEs Research in India
The PIECEs arts team in India successfully conducted a virtual workshop with 10 mental health professionals from SCARF India on 6th and 7th July 2021. Here is what the workshop leader Ms. Mrithula Chetlur has to say about the workshops
Interviewer: Hi Mrithula, you did a great job leading the mental health professionals (MHP) workshop. How did you find it?
Mrithula: Actually I came on board not knowing whether I’ll have to be an actor or a joker. So when I was asked to be one, I thought it was interesting to see what would come up in the field of mental health. From few initial trainings I definitely was aware that it was a little larger world that I would be interacting with. So it was both incredible excitement and quite a bit of responsibility. Also I was aware that the cultural relevance of what we were doing was important. The fact that we are regionalising and rooting the workshop to our culture was so exciting for me.
I: Did you get what you wanted from this workshop?
Mrithula: It gave me more than I expected. Doing it with MHPs alone was tremendous and I know we are going to explore a more unknown world when we do this with the caregivers and the patients
I: What did you observe about participant contribution?
Mrithula: I would like to appreciate the time and effort that the Clinicians put in to participate in the workshop, understanding how valuable each of their time is. I was pleasantly surprised at their openness to share and how they quickly grasped what we were looking for from them. They were very open to bringing their perspectives into the conversation.

I: You have lead a lot of workshops in different settings. How different was this workshop when compared to others?
Mrithula: In other workshops we are working with worlds that we are kind of aware of. For example the themes and the type of stories which they share. But here, we saw how the MHPs involvement in their clients lives influences the conversations that we had. We saw that they are a lot more intricately involved in their clients lives personally. Also when we did one exercise where the MHPs have to act out a scenario, we saw how they were cued in to ask questions and get to know the client more. It usually happens with us the facilitators but to have that from the other side was very interesting.
I: The MHP appeared to enjoy the games you had for them. Did you get what you wanted from the workshops?
Mrithula: Yes we had few themes which we thought was important. But we were open because this is one workshop where we were going to gain information than to impart. This was a catalyst to gain more from the people’s experience. So whatever came out was fodder for us. We also got few surprises, for instance when we did the monologues on the second day, where the conversation took us was very interesting for us, that was exactly what we wanted see how a trigger would take us to different places as it makes understand what they have to handle. That way it was defined to have that fluidity and it did surprise us.
I: You did a good job of involving the participants in the activities. How did your team find balancing and managing time for all participants?
Mrithula: Paul and Sunil were incredibly helpful in handling this thought of balancing time for doing and talking. Coz at the end of the day the aim is to gain perspectives from their experiences. But in TO workshops there is a lot of importance in making participants ‘do’, as it makes the person get out of their head and in turn will make them share things which they normally might not. So how much to prioritize doing over sharing was constantly being reviewed as we were going through. So yes time management was of concern, understanding that people are short on time. Thoughts were on do we let everyone engage in everything. So we left it to them, if they wanted to share let them but if they are just reacting let them be and we didn’t want to pull anyone in.
I: Was language a factor which influenced the workshop?
Mrithula: Only when we thought we should do in Tamil. Though I speak in Tamil, certain conversations I have never had in Tamil and so I don’t know or am not used to using certain words or usages. Especially being someone who wants to have conversations to people to become aware of, I realised that certain conversations I haven’t had in Tamil. And even haven’t thought about them in that angle. It was actually a learning experience for me personally and I’ve become more mindful of it. But it was not a barrier in getting or sharing information on experiences.
I: Are there things you are planning to change for the next two workshops with patients and caregivers from your experience with the MHP?
Mrithula: There is already an ongoing discussion to keep the basics same and to tweak the monologues and scenarios for the next two workshops to bring out life related themes. So yes there are certain changes which we are planning.
I: On a scale of 0-10 how satisfied were you in conducting this workshop?
Mrithula: I think our goal was to know more of the life of the people attending and to know them more personally. Having that in mind I never give 10 on 10 for any scale because there is nothing which is perfect. So I would give a 9.5 on 10 for the workshop which happened.
I: Thank you so much, Mrithula, for your time.
Mrithula: Thank you.

First Impressions as an Observer: Arts Workshops as part of PIECEs Research
*written by Hufsa Sarwar – PIECEs Research Coordinator in Pakistan
Pakistan has a rich history of arts and drama, however, even in 2021 theatre as an art form has not been able to integrate into the mainstream entertainment circles. It has unfortunately either been associated with taboo ideas and behaviours, or is available to a few privileged groups in society. Knowing this, I felt extremely apprehensive about organising Theatre of the Oppressed workshops – a new concept within mental health – for healthcare providers, caregivers, and people with lived experience of psychosis. Even if they agreed to be a part of the sessions, would they be able to leave behind their inhibitions and play with us while sharing their personal stories?

Healthcare workers during Theatre of the Oppressed Arts Workshops
Convincing our desired demographic to attend the workshops proved to be a long and gruelling process. People were unable to comprehend how games and exercises would help with furthering the understanding of the experience of psychosis in Pakistan. Thankfully, we were able to enrol a sufficient number of participants from each of the three groups, and kicked off the first set of workshops with psychiatrists and psychologists. Contrary to my expectations, the seemingly serious healthcare providers broke away from the confines of their professions, and took part in the games without reservations, sharing poignant stories and experiences from their clinical work. Led by our Arts partners from IRC (Interactive Resource Centre), some of the images created showed their struggle with burnout, lack of availability of support staff at hospitals, the importance of family counselling, and the great need for support groups for caregivers of people with psychosis. We received positive feedback from all the healthcare providers, who shared that they were usually so entrenched within their daily routines and structures that they were unable to view the experiences of patients and caregivers from the different perspective that Theatre of the Oppressed provided.

We decided to hold workshops with caregivers and people with psychosis together in the same room due to challenges around attendance. These individuals surprised me with how generous they were with their stories and challenges, and how brilliantly they communicated through the games and exercises. Initially, the caregivers exhibited some resistance; however, once they saw their family members and others with psychosis enthusiastically taking part in the activities, they decided to loosen up as well. Most participants with psychosis shared that they expected to feel better after these workshops, and that they wanted to learn something new. Most caregivers said they were there because of their family member, and wanted to learn how to better support them. By the end of the second day, the entire group came together and constructed powerfully evocative images of being restrained by their family members when experiencing active symptoms of psychosis, the challenge of seeking care at overburdened hospitals, the overwhelming responsibility and subsequent stress faced by caregivers, and the need for increased empathy and understanding of the condition.

The stories and experiences that our participants shared have opened up a myriad of questions around the challenges faced by those living with psychosis, their family members, as well as the healthcare providers who work with them. We hope to work with these stakeholders to further develop these stories, and bring them to the wider community to raise awareness and increase acceptance and understanding of psychosis in Pakistan.
To finalise, read the impressions from Dr. Faiza Rehman, Psychiatrist at Jinnah Postgraduate Medical Centre (JPMC), regarding her participation on the Arts Workshops:
I registered for the workshop with a lot of curiosity, to be honest. It was almost serendipitous for me that art forms were being utilised in the management of mental health. Although this isn’t a new concept, it is now not only being implemented in Pakistan but is also within reach. It was a thoroughly refreshing experience and I will take the liberty to say that I was there partly to cater my own cravings for performing arts and being able to be of some help for others, in that process, was a double fold joy in itself. Although the moderating team and my fellow participants met each other for the first time, the bond that was formed between them and the experience gained was such a positive one – probably due to the goodness of intent and nobility of the cause that brought them together. The workshop helped us see the small details of patient care and even the perspectives of a caregiver that might get neglected in the routine hassle of managing the patient. With a lot of heartfelt wishes for the team managing this project I look forward to more such activities and would be eager to be a part of them in the future.

First Impressions: Using DIALOG+ in PIECEs pilot phase
*written by Dr. Padmavati Ramachandran, Co-Investigator on PIECEs and Director at Schizophrenia Research Foundation (SCARF)
Psychosocial interventions, that impact recovery for persons with psychosis, are contingent upon several aspects – the person with psychosis, family, the care provider, available resources and in all likelihood, the passage of time! Hence, development of a new comprehensive intervention in the field of psychosocial interventions is in itself a challenge and testing the intervention even more so.
The DIALOG + an intervention designed to promote better patient-clinician interaction, brings in a structure to the conversations in routine clinical interactions. Being a part of the team piloting the tool at SCARF, it became very clear, right at the outset that tool was actually facilitating a dialogue with the patient that would not just improve conversation , but also facilitate a solution focussed discussion.
The first participant, a 43 year old women, was someone I have occasionally met in clinical encounters. She would always complain that she had a lot to speak about – but the doctors were so busy in the OPD, that she didn’t think it was right for her to take more time. The first session with the app – actually left her feeling that she was listened to – in her own words “l feel that for the first time – I have said all that has been bothering me in terms of my functioning” And, she adds, “you have spoken to me and not my husband… that makes me feel even better”
One interesting observation with the third participant was something that I least anticipated. In the domain related to Job situation – the participant a home maker, spontaneously stated that her action plan would be to learn to create an email id for herself – so that she can apply for jobs. This was something that was never picked up during clinical interactions! Similarly, a male participant who works as a tailor, who wanted to feel more energetic – reported that he could exercise and we then engaged in a discussion of what he could do to exercise. He left the session , saying that he liked the idea of exercising – an activity that he had not thought of before!
The experience of handling a gadget – the tablet in this case – is a very new experience, even for me as a clinician! While I do use the electronic medical records system for client data storage, using the tablet as a medium to communicate to the client is quite a task, especially when the participant is not very familiar with using the electronic medium. But as I realised over the next few sessions , it was a matter of practice.
The app driven technology is very user friendly and simple. This enables the participant to be able to read and relate easily to the visual analogue scale. The use of the Tamil language has made the interaction even more suitable! There are of course, sections that will need adaptation to the Indian lifestyle and the PIECES project aims to do just that!
Overall, I feel pretty excited at using this tool – it has brought in a structure to a patient centric engagement, meaningful enough to hopefully improve on functioning.
Alongside with Dr. Padmavati’s first impressions in India, in Pakistan Dr. Aneela Mushtaq , clinical psychologist at hospital Karwan-e-Hayaat, gives her account of the experience with the intervention so far:
Since I have started using DIALOG+, I have found this exceptional intervention, convenient for both therapist and patient; reliable, time-saving and specific in targeting the main issue which is causing distress. It helps both therapist and patient to understand problems in more depth. Before, both sides had to do a lot of paperwork during psychotherapy sessions, however ever since I have started utilising DIALOG+ in my therapy sessions, my paperwork has noticeably decreased. If I talk about my patients’ views regarding DIALOG+ – according to them it is very easy to work with the instrument, and they can easily highlight the core issue which is the main source of problems. Previously both the therapist and the patient needed to take part in four to five sessions to come to the conclusion of the main problem, as normally either we are doing it verbally or performing some paperwork for clear understanding. Furthermore, another very effective part of the intervention is the action plan. This option helps to form smart goals for the rest of the week: patients have to achieve those goals while working on it.
To understand more about DIALOG+ and how it’s used, please access the official website
Reflexive Analysis: Clinical sciences & the other sides, coming together for a common goal
*written by Kausar Khan, Co-I in PIECEs, social scientist and expert in community engagement
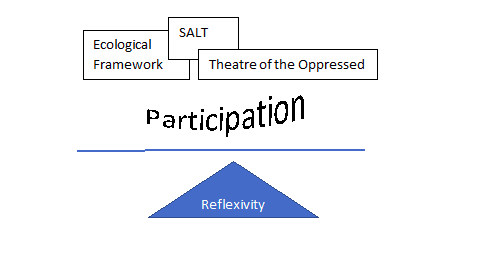
The clinician, armed with scientific know how, is well equipped to deal with the medical side of psychosis, but the challenges rises from the socio-cultural context of the patient with psychosis. The patient is not alone, his/her family is vested in the well being of the patient. The optimal use of clinical sciences becomes possible with the help of reflexivity, ecological framework, meaning of participation, SALT, Theatre of the Oppressed
Reflexivity is an honest act, & you are its sole witness. The reflexive practitioners examines their own attitudes and assumptions that shape their teaching/learning methods, and thus continually improve their experiences and learn from them. To become reflexive, you must begin to practice reflexivity
The ecological framework draws attention to the relationships between individuals and their families, and the individual/families with their communities/neighbourhood. A patient with psychosis, like any individual, is caught in a web of relationship s. Medical treatment of an individual has to be nested in the understanding of the family, neighbourhood and social norms that control individuals and families.
Participation. What is the nature of participation of a patient and his/her family in the wellbeing of the patient? Participation is a central concept in primary health care, as well as in all community development efforts. Typology of Participation helps understand this notion, and also reflect on the type pursued in one’s work. SALT is committed to the type of participation/engagement that would be based on community’s ownership of the issue; and taking action to take forward their aspirations/dream. Theatre of the Oppressed, ideologically resonating SALT’s aspirations of ownership, uses powerful theatre-techniques developed by the founders of this approach.
For further resources on the subject, this article might also be useful.
